|
|
|
| Referral coordination mechanism of gatekeeper healthcare system |
Yue ZHANG( ),Zhao GAO,Na LI*() ),Zhao GAO,Na LI*() |
| School of Mechanical Engineering, Shanghai Jiao Tong University, Shanghai 200240, China |
|
|
|
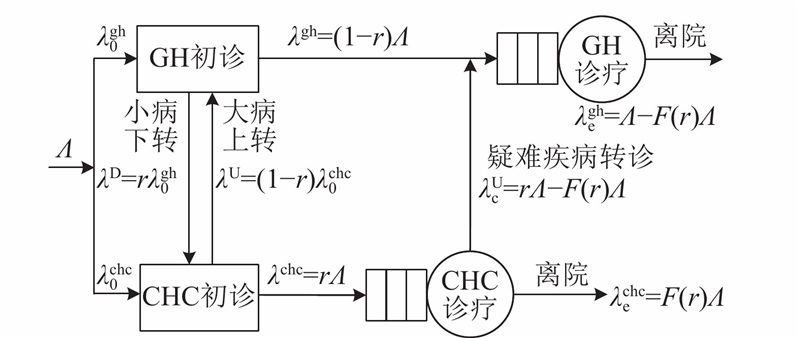
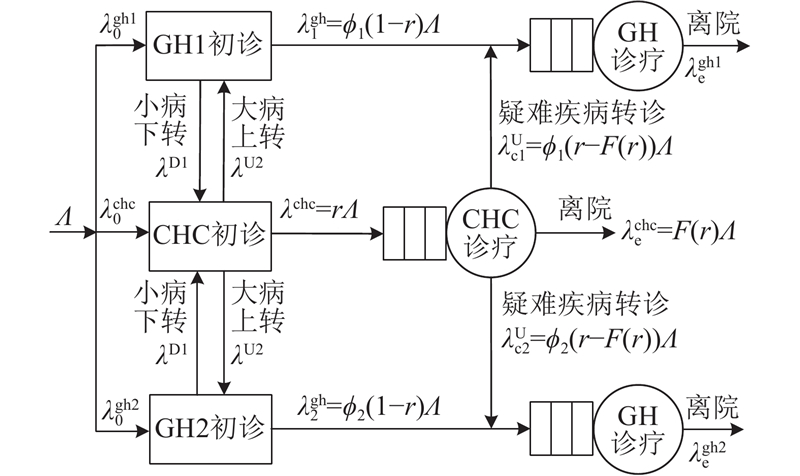
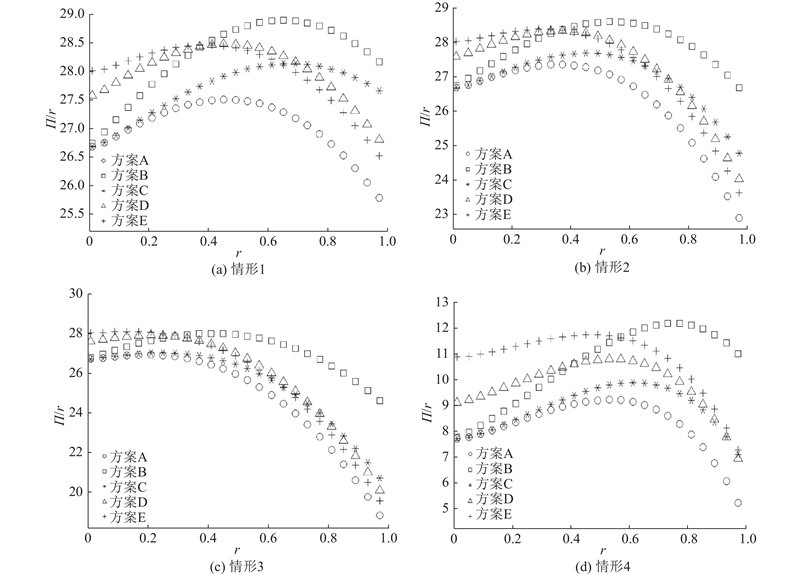
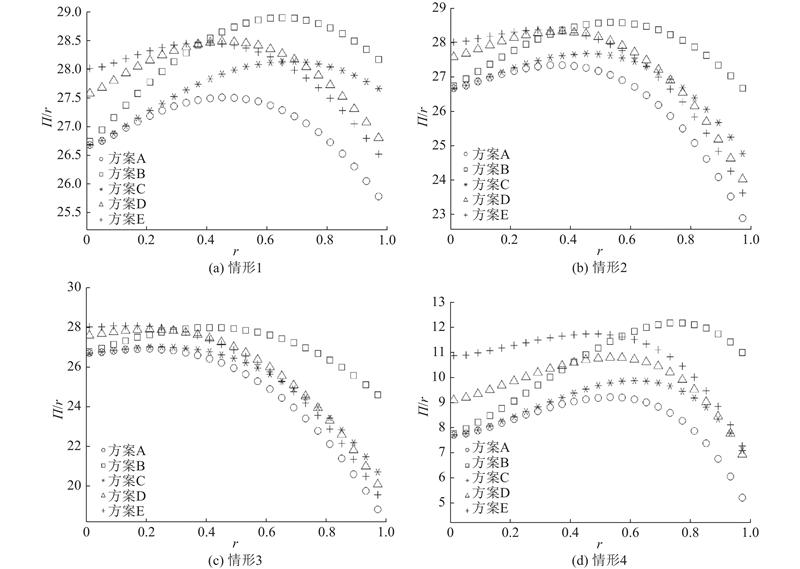
Abstract A referral model with general hospitals (GH) and community health centers (CHC) was established to analyze the coordination problem of the gatekeeper healthcare system. The non-competitive and competitive models respectively studied the optimal referral strategies and the optimal contract forms from centralized decision-making and service payment contract cooperation, and provided the conditions for system coordination. Results show that reducing the unit service costs in the system can effectively improve the system, and competition can increase the referral threshold to promote community first diagnosis. The non-competitive and competitive systems for service payment contract coordination at different scales are feasible. The coordination efficiency of small-scale is better than that of large-scale in competitive system, then designing multiple small competitive hospitals can bring higher social efficiency.
|
|
Received: 09 December 2019
Published: 31 December 2020
|
|
|
|
Corresponding Authors:
Na LI
E-mail: zy_0036@sjtu.edu.cn;nali-03@sjtu.edu.cn
|
“守门人”医疗系统中的转诊协调机制
为了探究“守门人”医疗系统的协调问题,建立系统内综合医院与社区医院间的转诊博弈模型,分别对非竞争型和竞争型的2种系统建模. 模型分别研究系统集中决策下的最优转诊阈值策略以及服务支付契约合作模式下的最优契约形式. 结论表明,降低系统内单位人员服务成本能够有效提升系统效用,引入竞争可以降低转诊率、促进社区医院首诊;非竞争与竞争型系统在不同规模下的服务支付契约对于实现系统协调均具有可行性,竞争系统下小规模设置的协调效率高于大规模设置的. 在医疗系统设计中若无法避免竞争的存在,设置多个小型竞争医院能带来更高的社会效率.
关键词:
“守门人”系统,
医疗系统,
转诊博弈,
协调机制,
竞争
|
|
| [1] |
张雪, 田文华 家庭医生制度的“守门人”作用及对我国的启示[J]. 中国社会医学杂志, 2013, 30 (2): 115- 117
ZHANG Xue, TIAN Wen-hua Effects of gatekeeper and inspirations of the family physician system in China[J]. Chinese Journal of Social Medicine, 2013, 30 (2): 115- 117
|
|
|
| [2] |
张淑娥, 孙涛 荷兰医改及对我国构建整合型健康服务体系的启示[J]. 中国卫生政策研究, 2019, 12 (8): 15- 22
ZHANG Shu-e, SUN Tao The netherland health reform experiences and its enlightenment for the construction of China’s integrated healthcare service system[J]. Chinese Journal of Health Policy, 2019, 12 (8): 15- 22
doi: 10.3969/j.issn.1674-2982.2019.08.003
|
|
|
| [3] |
SHUMSKY R A, PINKER E J Gatekeepers and referrals in services[J]. Management Science, 2003, 49 (7): 839- 856
doi: 10.1287/mnsc.49.7.839.16387
|
|
|
| [4] |
LI N, TENG D, KONG N Threshold control policy optimization for real-time reverse referral decision of Chinese comprehensive hospitals[J]. IEEE Transactions on Automation Science and Engineering, 2018, 16 (1): 45- 60
|
|
|
| [5] |
QIU Y, SONG J, LIU Z A simulation optimisation on the hierarchical health care delivery system patient flow based on multi-fidelity models[J]. International Journal of Production Research, 2016, 54 (21): 6478- 6493
doi: 10.1080/00207543.2016.1197437
|
|
|
| [6] |
LI N, KONG N, LI Q, et al Evaluation of reverse referral partnership in a tiered hospital system: a queuing-based approach[J]. International Journal of Production Research, 2017, 55 (19): 5647- 5663
doi: 10.1080/00207543.2017.1327731
|
|
|
| [7] |
HASIJA S, PINKER E J, SHUMSKY R A Staffing and routing in a two-tier call center[J]. International Journal of Operational Research, 2005, 1 (1/2): 8- 29
doi: 10.1504/IJOR.2005.007431
|
|
|
| [8] |
LEE H H, PINKER E J, SHUMSKY R A Outsourcing a two-level service process[J]. Management Science, 2012, 58 (8): 1569- 1584
doi: 10.1287/mnsc.1110.1503
|
|
|
| [9] |
LIU X, CAI X, ZHAO R, et al Mutual referral policy for coordinating health care systems of different scales[J]. International Journal of Production Research, 2015, 53 (24): 7411- 7433
doi: 10.1080/00207543.2015.1082039
|
|
|
| [10] |
GAO X, WEN J, SONG J Capacity allocation and revenue sharing in healthcare alliances[J]. Flexible Services and Manufacturing Journal, 2019, (2): 1- 23
|
|
|
| [11] |
ADIDA E, BRAVO F Contracts for healthcare referral services: coordination via outcome-based penalty contracts[J]. Management Science, 2018, 65 (3): 1322- 1341
|
|
|
| [12] |
BICHESCU B C, BRADLEY R V, SMITH A L, et al Benefits and implications of competing on process excellence: evidence from California hospitals[J]. International Journal of Production Economics, 2018, 202: 59- 68
doi: 10.1016/j.ijpe.2018.05.013
|
|
|
| [13] |
CACHON G P Supply chain coordination with contracts[J]. Handbooks in Operations Research and Management Science, 2003, 11: 227- 339
doi: 10.1016/S0927-0507(03)11006-7
|
|
|
| [14] |
CACHON G P, LARIVIERE M A Supply chain coordination with revenue-sharing contracts: strengths and limitations[J]. Management Science, 2005, 51 (1): 30- 44
doi: 10.1287/mnsc.1040.0215
|
|
|
| [15] |
YAO Z, LEUNG S C H, LAI K K Manufacturer′s revenue-sharing contract and retail competition[J]. European Journal of Operational Research, 2008, 186 (2): 637- 651
doi: 10.1016/j.ejor.2007.01.049
|
|
|
| [16] |
GUO L, WU X Capacity sharing between competitors[J]. Management Science, 2017, 64 (8): 3554- 3573
|
|
|
| [17] |
周健, 张玉华 传统零售商渠道选择策略微分博弈模型[J]. 浙江大学学报: 工学版, 2019, 53 (9): 1720- 1727
ZHOU Jian, ZHANG Yu-hua Differential game model for channel selection strategies of traditional retailer[J]. Journal of Zhejiang University: Engineering Science, 2019, 53 (9): 1720- 1727
|
|
|
| [18] |
秦星红, 李海南, 曹园园. 多服务商竞争环境下考虑利润公平分配的网购服务供应链激励契约[EB/OL]. [2020-02-21]. http://kns.cnki.net/kcms/detail/31.1738.T.20191223.1427.002.html.
|
|
|
| [19] |
邓晨卉, 潘杰 医院市场竞争与不同严重程度疾病医疗费用关系的比较研究?基于行手术治疗的腰椎间盘突出和老年性白内障住院病例的实证分析[J]. 现代预防医学, 2019, 46 (23): 4293- 4297
DENG Chen-hui, PAN Jie Comparative study on the relationship between hospital competition and medical expenses for diseases with different severity?an empirical analysis based on inpatients of lumbar disc herniation and senile cataract treated by surgery[J]. Modern Preventive Medicine, 2019, 46 (23): 4293- 4297
|
|
|
| [20] |
周奕男, 熊雪晨, 何世英, 等 基于竞争和需求测算的社会办基层医疗机构空间布局导引方法实证研究[J]. 中国医院管理, 2019, 39 (8): 18- 19
ZHOU Yi-nan, XIONG Xue-chen, HE Shi-ying, et al Empirical study on layout guidance method for private grassroots medical institutions based on competition and demand calculation[J]. Chinese Hospital Management, 2019, 39 (8): 18- 19
|
|
|
| [21] |
匡莉 我国医疗服务竞争机制的优化策略——建立纵向整合的医疗服务体系[J]. 中国卫生政策研究, 2012, 5 (9): 34- 39
KUANG Li Strategy for optimizing the mechanism of healthcare competition: establishing the vertical integrated healthcare delivery systems[J]. Chinese Journal of Health Policy, 2012, 5 (9): 34- 39
doi: 10.3969/j.issn.1674-2982.2012.09.006
|
|
|
| [22] |
蔡立辉 分层次、多元化、竞争式: 我国医疗卫生服务的公共管理改革[J]. 中国人民大学学报, 2010, 24 (1): 92- 100
CAI Li-hui Public administration reform of medical health servicein a competitive way with multi-models and in multi-levels[J]. Journal of Renmin University of China, 2010, 24 (1): 92- 100
|
|
|
| [23] |
JIANG H J, FRIEDMAN B, JIANG S Hospital cost and quality performance in relation to market forces: an examination of U.S. community hospitals in the“post-managed care era”[J]. International Journal of Health Care Finance and Economics, 2013, 13 (1): 53- 71
doi: 10.1007/s10754-013-9122-9
|
|
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|