| Article |
|


|
|
|
| Concomitant coronary and renal revascularization improves left ventricular hypertrophy more than coronary stenting alone in patients with ischemic heart and renal disease |
Hao-jian Dong( ),Cheng Huang,De-mou Luo,Jing-guang Ye,Jun-qing Yang,Guang Li,Jian-fang Luo,Ying-ling Zhou() ),Cheng Huang,De-mou Luo,Jing-guang Ye,Jun-qing Yang,Guang Li,Jian-fang Luo,Ying-ling Zhou() |
| Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong General Hospital, Guangdong Academic of Medical Sciences, Guangzhou 510080, China |
|
|
|
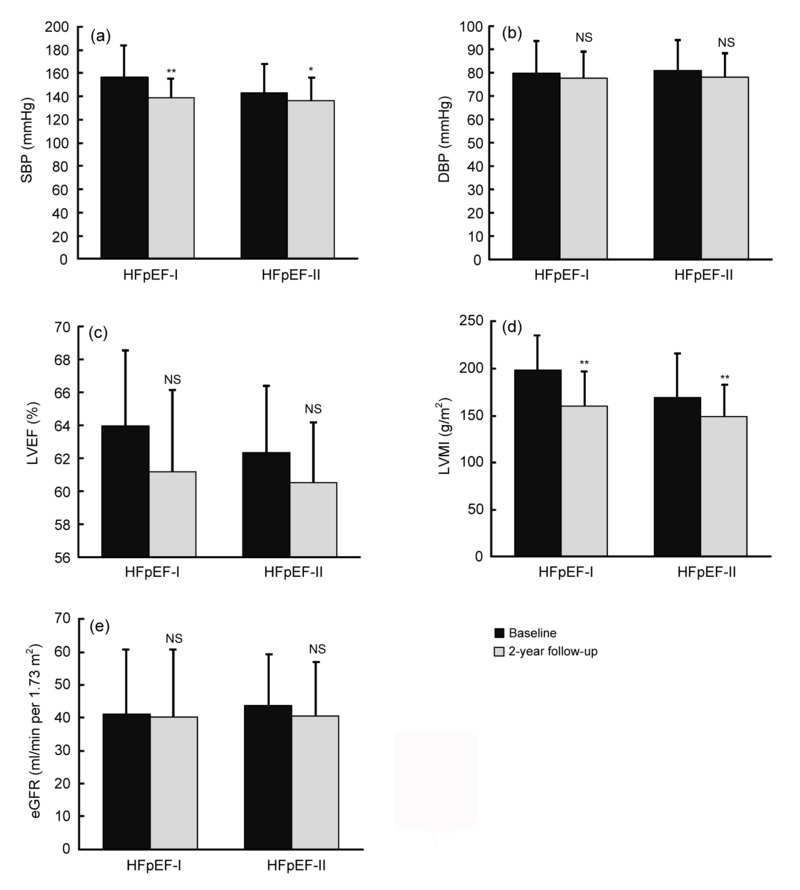
Abstract Percutaneous transluminal renal artery stenting (PTRAS) has been proved to have no more benefit than medication alone in treating atherosclerotic renal artery stenosis (ARAS). Whether PTRAS could improve left ventricular hypertrophy (LVH) and reduce adverse events when based on percutaneous coronary intervention (PCI) for patients with coronary artery disease (CAD) and ARAS is still unclear. A retrospective study was conducted, which explored the effect of concomitant PCI and PTRAS versus PCI alone for patients with CAD and ARAS complicated by heart failure with preserved ejection fraction (HFpEF). A total of 228 patients meeting inclusion criteria were divided into two groups: (1) the HFpEF-I group, with PCI and PTRAS; (2) the HFpEF-II group, with PCI alone. Both groups had a two-year follow-up. The left ventricular mass index (LVMI) and other clinical characteristics were compared between groups. During the follow-up period, a substantial decrease in systolic blood pressure (SBP) was observed in the HFpEF-I group, but not in the HFpEF-II group. There was marked decrease in LVMI in both groups, but the HFpEF-I group showed a greater decrease than the HFpEF-II group. Regression analysis demonstrated that PTRAS was significantly associated with LVMI reduction and fewer adverse events after adjusting for other factors. In HFpEF patients with both CAD and ARAS, concomitant PCI and PTRAS can improve LVH and decrease the incidence of adverse events more than PCI alone. This study highlights the beneficial effect of ARAS revascularization, as a new and more aggressive revascularization strategy for such high-risk patients.
|
|
Received: 23 March 2015
Published: 01 January 2016
|
| Fund: Project supported by the Guangdong Provincial Scientific Grant, China(No. 2013B031800024) |
|
Corresponding Authors:
Hao-jian Dong,Ying-ling Zhou
E-mail: donghaojian@sina.com;zylgdh@163.com
|
|
|
| [1] |
Asrar ul Haq M, Wong C, Mutha V. Therapeutic interventions for heart failure with preserved ejection fraction: a summary of current evidence. World J Cardiol. 2014, 6(2):67-76. (Available from: http://dx.doi.org/10.4330/wjc.v6.i2.67)
doi: 10.4330/wjc.v6.i2.67
pmid: 24575173
|
|
|
| [2] |
Chábová V, Schirger A, Stanson AW. Outcomes of atherosclerotic renal artery stenosis managed without revascularization. Mayo Clin. Proc. 2000, 75(5):437-444. (Available from: http://dx.doi.org/10.4065/75.5.437)
doi: 10.4065/75.5.437
|
|
|
| [3] |
Chobanian AV, Bakris GL, Black HR. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003, 42(6):1206-1252. (Available from: http://dx.doi.org/10.1161/01.HYP.0000107251.49515.c2)
doi: 10.1161/01.HYP.0000107251.49515.c2
|
|
|
| [4] |
Cooper CJ, Murphy TP, Cutlip DE. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014, 370(1):13-22. (Available from: http://dx.doi.org/10.1056/NEJMoa1310753)
doi: 10.1056/NEJMoa1310753
pmid: 4815927
|
|
|
| [5] |
Dean RH, Kieffer RW, Smith BM. Renovascular hypertension: anatomic and renal function changes during drug therapy. Arch Surg. 1981, 116(11):1408-1415. (Available from: http://dx.doi.org/10.1001/archsurg.1981.01380230032005)
doi: 10.1001/archsurg.1981.01380230032005
|
|
|
| [6] |
de Silva R, Nikitin NP, Bhandari S. Atherosclerotic renovascular disease in chronic heart failure: should we intervene?. Eur Heart J. 2005, 26(16):1596-1605. (Available from: http://dx.doi.org/10.1093/eurheartj/ehi304)
doi: 10.1093/eurheartj/ehi304
pmid: 15919719
|
|
|
| [7] |
Ding J, Xu H, Yin X. Estrogen receptor α gene PvuII polymorphism and coronary artery disease: a meta-analysis of 21 studies. J Zhejiang Univ-Sci B (Biomed & Biotechnol). 2014, 15(3):243-255. (Available from: http://dx.doi.org/10.1631/jzus.B1300220)
doi: 10.1631/jzus.B1300220
pmid: 24599688
|
|
|
| [8] |
Folland ED, Parisi AF, Moynihan PF. Assessment of left ventricular ejection fraction and volumes by real-time, two-dimensional echocardiography. A comparison of cineangiographic and radionuclide techniques. Circulation. 1979, 60(4):760-766. (Available from: http://dx.doi.org/10.1161/01.CIR.60.4.760)
doi: 10.1161/01.CIR.60.4.760
|
|
|
| [9] |
Ghanami RJ, Rana H, Craven TE. Diastolic function predicts survival after renal revascularization. J Vasc Surg. 2011, 54(6):1720-1726. (Available from: http://dx.doi.org/10.1016/j.jvs.2011.05.091)
doi: 10.1016/j.jvs.2011.05.091
pmid: 3230744
|
|
|
| [10] |
Groban L, Kitzman DW. Diastolic function: a barometer for cardiovascular risk. Anesthesiology. 2010, 112(6):1303-1306. (Available from: http://dx.doi.org/10.1097/ALN.0b013e3181da89e4)
doi: 10.1097/ALN.0b013e3181da89e4
pmid: 3057510
|
|
|
| [11] |
Hirsch AT, Haskal ZJ, Hertzer NR. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J Am Coll Cardiol. 2006, 47(6):1239-1312. (Available from: http://dx.doi.org/10.1016/j.jacc.2005.10.009)
doi: 10.1016/j.jacc.2005.10.009
|
|
|
| [12] |
Kane GC, Xu N, Mistrik E. Renal artery revascularization improves heart failure control in patients with atherosclerotic renal artery stenosis. Nephrol Dial Transplant. 2010, 25(3):813-820. (Available from: http://dx.doi.org/10.1093/ndt/gfp393)
doi: 10.1093/ndt/gfp393
pmid: 19666661
|
|
|
| [13] |
Levy D, Garrison RJ, Savage DD. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990, 322(22):1561-1566. (Available from: http://dx.doi.org/10.1056/NEJM199005313222203)
doi: 10.1056/NEJM199005313222203
|
|
|
| [14] |
Little WC, Brucks S. Therapy for diastolic heart failure. Prog Cardiovasc Dis. 2005, 47(6):380-388. (Available from: http://dx.doi.org/10.1016/j.pcad.2005.02.004)
doi: 10.1016/j.pcad.2005.02.004
pmid: 16115517
|
|
|
| [15] |
Liu XB, Jiang JB, Zhou QJ. Evaluation of the safety and efficacy of transcatheter aortic valve implantation in patients with a severe stenotic bicuspid aortic valve in a Chinese population. J Zhejiang Univ-Sci B (Biomed & Biotechnol). 2015, 16(3):208-214. (Available from: http://dx.doi.org/10.1631/jzus.B1500017)
doi: 10.1631/jzus.B1500017
pmid: 25743122
|
|
|
| [16] |
Marcantoni C, Zanoli L, Rastelli S. Effect of renal artery stenting on left ventricular mass: a randomized clinical trial. Am J Kidney Dis. 2012, 60(1):39-46. (Available from: http://dx.doi.org/10.1053/j.ajkd.2012.01.022)
doi: 10.1053/j.ajkd.2012.01.022
pmid: 22495466
|
|
|
| [17] |
McMurray JJ, Adamopoulos S, Anker SD. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012, 14(8):803-869. (Available from: http://dx.doi.org/10.1093/eurjhf/hfs105)
doi: 10.1093/eurjhf/hfs105
|
|
|
| [18] |
Middleton RJ, Parfrey PS, Foley RN. Left ventricular hypertrophy in the renal patient. J Am Soc Nephrol. 2001, 12(5):1079-1084
doi: 10.1089/089277901300189538
pmid: 11316868
|
|
|
| [19] |
Park S, Jung JH, Seo HS. The prevalence and clinical predictors of atherosclerotic renal artery stenosis in patients undergoing coronary angiography. Heart Vessels. 2004, 19(6):275-279
doi: 10.1007/s00380-004-0789-1
pmid: 15799174
|
|
|
| [20] |
Patel SS, Kimmel PL, Singh A. New clinical practice guidelines for chronic kidney disease: a framework for K/DOQI. Semin Nephrol. 2002, 22(6):449-458
|
|
|
| [21] |
Przewlocki T, Kablak-Ziembicka A, Tracz W. Renal artery stenosis in patients with coronary artery disease. Kardiol Pol. 2008, 66(8):856-862 863-864
pmid: 18803137
|
|
|
| [22] |
Ronco C, di Lullo L. Cardiorenal syndrome. Heart Fail Clin. 2014, 10(2):251-280. (Available from: http://dx.doi.org/10.1016/j.hfc.2013.12.003)
doi: 10.1016/j.hfc.2013.12.003
|
|
|
| [23] |
Simon JF. Stenting atherosclerotic renal arteries: time to be less aggressive. Cleve Clin J Med. 2010, 77(3):178-189. (Available from: http://dx.doi.org/10.3949/ccjm.77a.09098)
doi: 10.3949/ccjm.77a.09098
|
|
|
| [24] |
Su CS, Liu TJ, Tsau CR. The feasibility, safety, and mid-term outcomes of concomitant percutaneous transluminal renal artery stenting in acute coronary syndrome patients at high clinical risk of renal artery stenosis. J Invasive Cardiol. 2013, 25(5):212-217
doi: 10.1186/1532-429X-15-35
pmid: 23645044
|
|
|
| [25] |
Wang X, Shi LZ. Association of matrix metalloproteinase-9 C1562T polymorphism and coronary artery disease: a meta-analysis. J Zhejiang Univ-Sci B (Biomed & Biotechnol). 2014, 15(3):256-263. (Available from: http://dx.doi.org/10.1631/jzus.B1300088)
doi: 10.1631/jzus.B1300088
pmid: 3955912
|
|
|
| [26] |
Wheatley K, Ives N, Gray R. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009, 361(20):1953-1962. (Available from: http://dx.doi.org/10.1056/NEJMoa0905368)
doi: 10.1056/NEJMoa0905368
pmid: 19907042
|
|
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|